

1. Sensory sensitivities
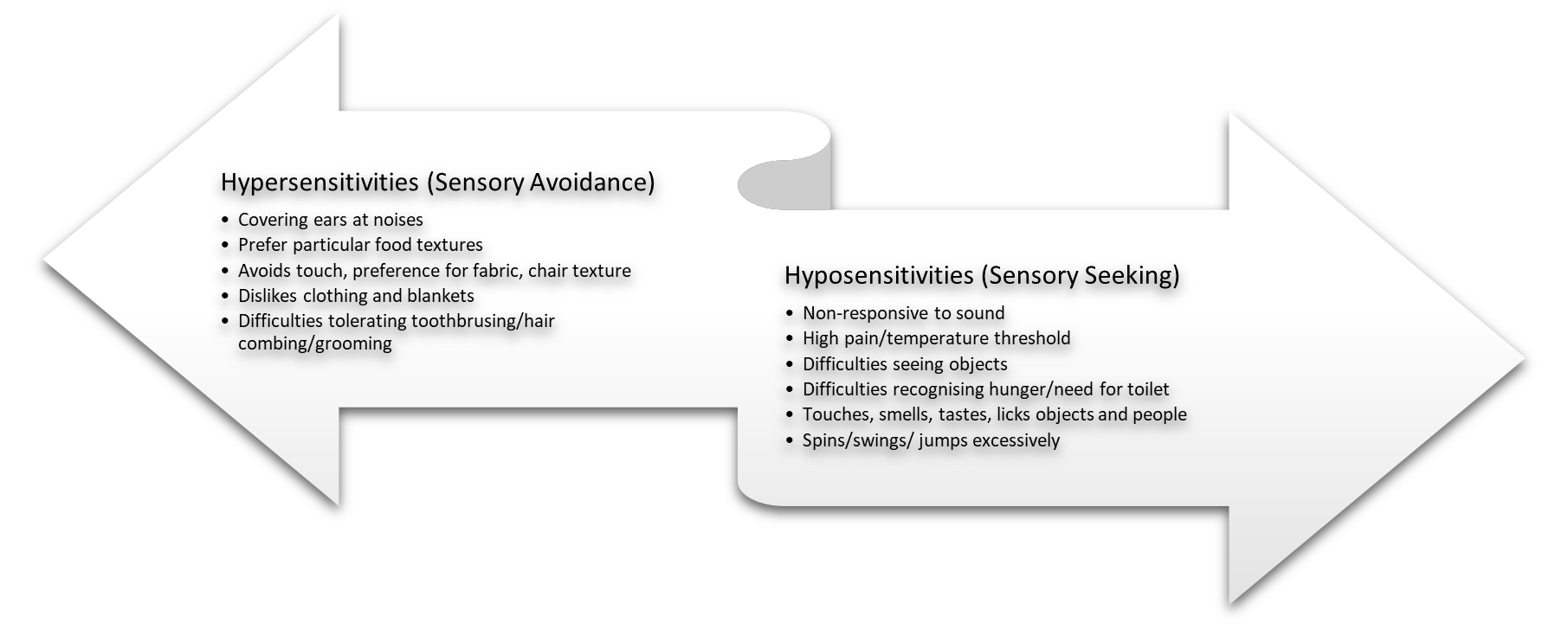
Hyper/Hypo sensitivities
Challenges with sensitivities come from sensory interaction with the environment and interpretation thereof. While these sensitivities fall on a continuum, many individuals with autism experience these on two extremes—hyper (overly) or hypo (low) sensitivity to sensory experiences. The hypersensitivities are often recognised as “sensory avoiders” require very light sensory stimulation in the senses to experience a reaction. Those with hyposensitivities, often referred to as “sensory seekers” may not react to sensory stimuli because it is poorly registered or recognised to elicit a reaction. Examples of hyper/hypo sensitivities may include but not limited to the following;
2. Fine and Gross Motor Difficulties
- Clumsiness and poor handwriting
- Problems with adaptive functioning
- Personal care and independent living skills
Theory of Mind
Theory of Mind (ToM) refers to the ability to put oneself in another’s shoes, literally taking their cognitive, emotional and visual perspective. This process equips children with skill for social interaction, group dynamics and behavior (Peterson, Slaughter, Peterson & Premack, 2013). For autism, the inability to appreciate the group perspective produces mind-blindness as a result, many people with autism experience difficulties understanding emotions, thoughts and intentions in themselves and others (Baron-Cohen, 1995). By adolescence, most individuals with Autism would pass a basic ToM test and are likely to be aware of the factual information known by another. However, they have difficulties to imagine the ways in which the other person perceives the factual information, or the emotions that they have in response to it. Major ways in which the Theory of Mind impairs social communication is illustrated in Figure 4 below:

3. Central Coherence
Central coherence (CC) is the ability to integrate pieces of information into a whole (Happe & Frith, 1996). With very weak central coherence, a person with Autism focuses on details without attending to the central meaning. Strong central coherence enables someone to comprehend and remember the gist of a conversation, story or situation and to integrate multiple cues to get a sense of the whole. Weak central coherence can impact the young person in a number of ways:
Weak central coherence
- If every detail is important, changes to the environment might be overwhelming.
- If someone remembers where everything is placed, moving things around maybe a source of distress.
- Challenges to integrating multiple stimuli might lead to difficulty noticing and responding to others’ emotions.
- If every detail is important, a change may result in something that has to be learned new, rather than being understood as something that is essentially similar
- The ability to generalise is difficult.
- Challenges attending to and integrating a range of types of cues, rather than the ‘whole’ of a social scene might lead to misinterpretation, faulty conclusions and eventual inappropriate solutions.
4. Executive Functioning
Executive functions (EF) refer to higher-order cognitive processes such as the ability to adapt behaviour to a changing situation, to plan and organise future behaviour, and to think abstractly. It is important to recognise that challenges in cognitive deficits are not permanent. Research shows that interventions in childhood, as well as family adaptation and individual compensatory strategies, make deficits less intrusive in adolescence. Below are executive function difficulties in autism;
- Planning and organisation
- Predicting ahead and planning to achieve a desired outcome, or avoid a pitfall.
- Concentrating, dividing attention, or shifting attention from one activity to another.
- Impulse control problems: knowing how to start and stop particular
- Getting started with a task or conversation.
- Reflecting on past experiences and adapting what has worked or did not
- Understanding the passage of time particularly trouble estimating time frames, losing track of time, prolonging a conversation topic or having particular expectations about start and end times for sessions.
- Adapting to new situations.